
If episodic care cannot fully address a continuous crisis, the next question is practical: what would it take to redesign systems around stability, and why has that proven difficult?
The constraint is not a lack of medical knowledge. It might be a structural time misalignment.
Non-communicable diseases (NCDs) account for roughly 74% of global deaths, which are more than 43 million annually. Over 80% of premature NCD deaths occur in low- and middle-income countries. Hypertension affects approximately 1.4 billion adults worldwide, yet global control rates remain near 21%. Cardiovascular disease accounts for roughly 19–20.5 million deaths each year. Uncontrolled blood pressure contributes to more than 10 million deaths annually.
These conditions are often described as “lifestyle diseases.” Lifestyle risk does complicate prevention efforts. However, decades of clinical research demonstrate that sustained control of blood pressure, glucose, and cholesterol is associated with significant reductions in stroke, myocardial infarction, kidney failure, and disability. For example, a 10-mmHg reduction in systolic blood pressure is associated with roughly a 20% reduction in major cardiovascular events. Biological mechanisms are well understood, and effective medications are widely available.
The persistent gap lies less in knowledge than in sustained control.
Chronic disease unfolds over decades. Health financing typically operates on annual cycles. Political terms are short. Insurance contracts often reset yearly. The benefits of improved blood pressure control today may not be visible in reduced stroke incidence for several years. This creates an inherent tension between long-term risk reduction and short-term budgeting.
The distinction between episodic and longitudinal management is best understood as a difference in how risk evolves between encounters. Conceptually, the trajectories diverge over time, as illustrated below.
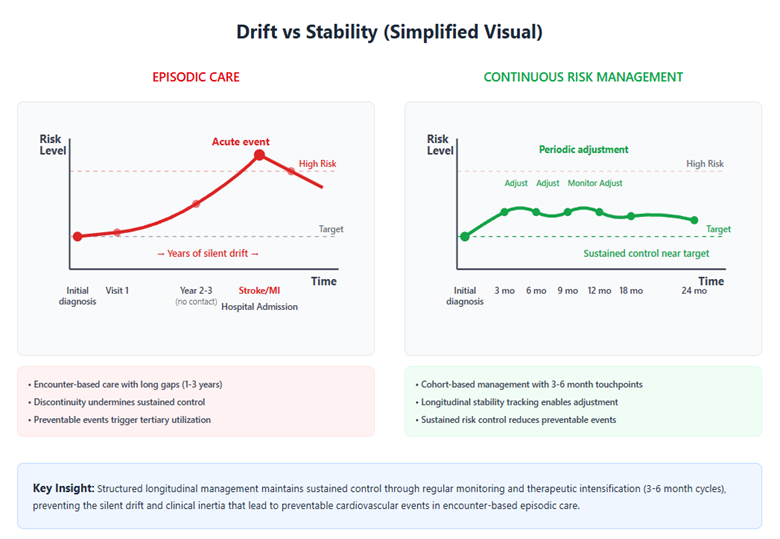
The simplified contrast above illustrates how differences in system design can influence risk trajectories over time. The literature identifies several recurring structural factors that help explain why episodic patterns persist.
Three structural patterns appear consistently in the literature.
First – Allocation patterns favor acute care
Hospitals account for 35–45% of health expenditure in many OECD countries, and in some middle-income settings, tertiary institutions absorb an even larger share. Primary care, where most chronic disease management occurs, often receives a comparatively smaller portion of spending. This allocation pattern reflects legitimate demands for acute and specialized services, but it may leave fewer resources for longitudinal risk management.
Second – Longitudinal stability is not consistently measured
Health systems reliably track admissions, procedures, and pharmaceutical volumes. Multi-year indicators such as sustained blood pressure control, medication persistence, or preventable cardiovascular admissions per 100,000 population are less consistently embedded in performance frameworks. When longitudinal control is not systematically tracked, deterioration may go unnoticed until acute events occur.
At this point, it is important to clarify the scope.
There is no single estimate of what proportion of global NCD burden is “fixable” through improved continuity of care, as determinants include policy, poverty, food environments, urban design, and individual behavior. However, evidence suggests that continuity of care influences several system-level factors associated with outcomes.
A major review of continuity of care in hypertension and diabetes reported that higher continuity was associated with reduced hospitalizations in 16 of 18 studies, reduced emergency visits in 8 of 8 studies, and lower mortality in 6 of 7 studies. WHO has estimated that long-term medication adherence for chronic diseases averages around 50% even in high-income countries and is often lower elsewhere. Separate analyses have shown that therapeutic intensification for uncontrolled hypertension occurs in only a minority of eligible visits.
Taken together, these findings suggest that a portion of preventable morbidity and utilization may be attributable to fragmentation, discontinuity, and clinical inertia, factors that are potentially responsive to structured longitudinal management. The evidence does not imply that continuity alone eliminates lifestyle risk, but it indicates that sustained engagement is associated with measurable differences in hospitalization, complication rates, and mortality.
Third – Equity gaps contribute to instability
In many low-income settings, out-of-pocket spending constitutes a substantial share of total health expenditure, creating barriers to sustained medication use. Rural populations may face weaker follow-up infrastructure. In high-income countries, discontinuation of chronic medications within the first year remains common. These patterns reflect structural friction rather than individual unwillingness alone.
Critiques that NCDs are primarily behavioral and therefore resistant to systems reform are partially valid. Behavior change is complex and influenced by socioeconomic and cultural factors beyond the health sector. At the same time, structured follow-up, adherence support, and timely treatment adjustment have been associated with improved control rates in multiple settings. Countries that report hypertension control rates above 50% typically combine guideline-based care with organized primary care follow-up systems rather than relying on episodic treatment alone.
The policy question, therefore, is not whether continuity alone solves NCDs. It is whether governance structures sufficiently support the sustained management of modifiable risk.
Several incremental approaches are plausible within existing systems:
- Adoption of a limited set of longitudinal stability indicators, such as 12-month blood pressure control or multi-year medication persistence. In practice, this could mean embedding 12-month blood pressure control as a standard reporting metric at the primary care network level, using data already captured in electronic records, rather than relying solely on visit-based indicators.
- Alignment of a modest portion of performance-based financing with sustained control metrics. Even allocating a small percentage of existing quality-linked payments to longitudinal control metrics would signal institutional priority without requiring wholesale restructuring.
- Gradual rebalancing of incremental budget growth toward primary and community-based management, where feasible.
- Stratification of outcomes by geography, income, and gender to ensure aggregate gains do not conceal widening disparities.
These adjustments would not be politically neutral. Budget reallocation, performance-based payment reforms, and expanded longitudinal tracking require institutional capacity, data infrastructure, and stakeholder alignment. Implementation would vary considerably across high-income and resource-constrained settings and would depend as much on political willingness as on technical feasibility.
Cardiovascular disease is estimated to cost the global economy over US$1 trillion annually. Even modest reductions in preventable events could translate into meaningful fiscal effects over time, although precise savings depend heavily on local context and implementation.
Technological capacity is less frequently cited as the primary constraint. Electronic records, risk stratification tools, and remote monitoring technologies are increasingly available. The more persistent challenge appears to be organizational: moving from encounter-based accounting to cohort-based management over time. Implementation would depend not only on data systems but also on primary care capacity and care coordination infrastructure, which vary substantially across settings.
This analysis does not suggest that stability metrics alone resolve lifestyle risk, nor that system reform eliminates structural determinants of disease. It suggests, more narrowly, that continuity of care is associated with measurable differences in outcomes and utilization, and that governance frameworks can either reinforce or undermine sustained risk control.
Chronic disease progresses gradually. That gradual trajectory can allow deterioration to accumulate unnoticed, but it also allows incremental improvement to compound.
The central question is not whether behavior is complex; it is whether systems are structured in budgeting, measurement, and accountability to support sustained management of that complexity over time.












